I found a tick. Now what?
If you've discovered a tick attached to your skin, you're probably wondering:
What should I do now?
Do I need treatment?
Should I ask for antibiotics?
The answer isn't as simple as you might expect.
Understanding your options after a tick bite
Many people assume there is one standard approach to treating a tick bite. In reality, there are two very different sets of medical guidelines for preventing and treating Lyme disease. As a result, two patients with the exact same tick bite could receive very different treatment recommendations.
Most hospitals, emergency departments, urgent care centers, and healthcare systems follow the guidelines developed by the Infectious Diseases Society of America (IDSA).
A second set of guidelines was developed by the International Lyme and Associated Diseases Society (ILADS), a nonprofit medical society dedicated to the diagnosis and treatment of Lyme disease and other tick-borne illnesses. Because most healthcare systems follow the IDSA guidelines, patients who wish to pursue care based on the ILADS guidelines may need to discuss those recommendations with their healthcare provider or seek care from a clinician who incorporates the ILADS guidelines into their practice.4
Understanding these differences can help you make informed decisions after a tick bite.
Two approaches at a glance
At the heart of these two guidelines is one fundamental question:
When a patient has a known tick bite, is it better to wait for signs of infection or begin treatment early while Lyme and other tick-borne diseases may still be preventable?
The IDSA and ILADS answer that question differently.
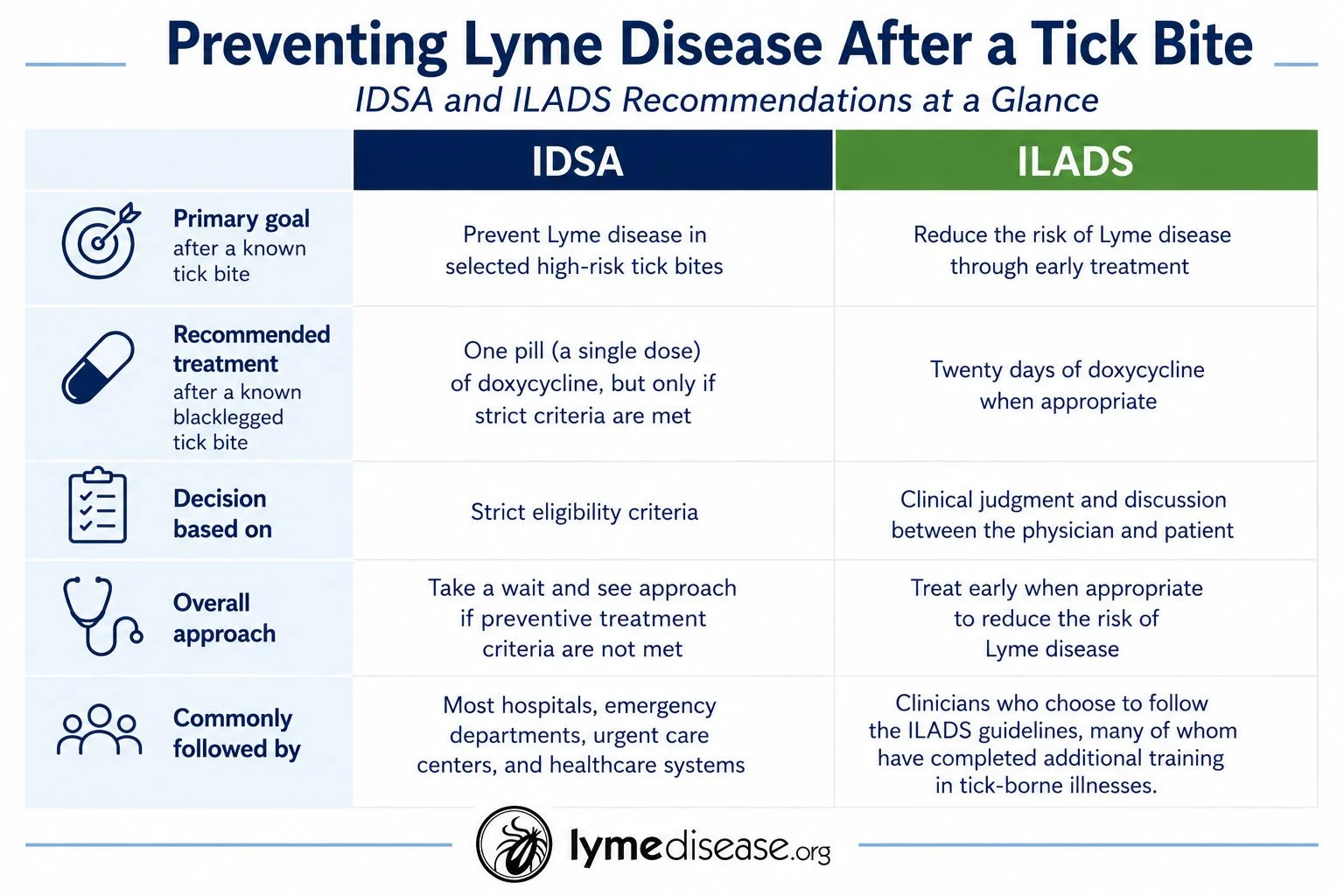
The IDSA approach
The IDSA recommends preventive treatment with one pill (a single dose) of doxycycline, but only after what it considers a high-risk blacklegged tick bite.
To qualify for preventive treatment under the IDSA guidelines, every one of the following criteria must be met:
• The tick is identified as a blacklegged (deer) tick.
• The tick is believed to have been attached for at least 36 hours.
• Treatment can begin within 72 hours of removing the tick.
• The bite occurred in an area where Lyme disease is considered common.
• Doxycycline is safe for the patient.
If any one of these criteria is not met, the IDSA recommends monitoring for symptoms rather than prescribing preventive antibiotics.
Why geography matters
One of the criteria used by the IDSA is where the tick bite occurred.
The CDC identifies several high-incidence states where Lyme disease is reported more frequently. Patients bitten in these states may qualify for preventive treatment if they also meet the remaining criteria as listed above.
High-incidence states include:
Connecticut
Delaware
District of Columbia
Maine
Maryland
Massachusetts
Minnesota
New Hampshire
New Jersey
New York
Pennsylvania
Rhode Island
Vermont
Virginia
West Virginia
Wisconsin
It is important to remember that Lyme disease and other tick-borne illnesses have now been reported in all 50 states, so there is risk in every state.3
Has the IDSA’s prevention recommendation kept pace?
The IDSA's recommendation for one pill of doxycycline after a qualifying high-risk tick bite has remained unchanged since 2006.6
During that same period, Lyme disease has become an increasingly common public health concern. Today, the Centers for Disease Control and Prevention (CDC) estimates that nearly 476,000 Americans are diagnosed and treated for Lyme disease each year.3
As Lyme disease has become more common, an important question has emerged:
Should prevention strategies evolve as well?
Why does ILADS recommend early treatment?
ILADS believes many of the factors used to determine whether a tick bite is considered "high risk" cannot be known with certainty.
Patients often do not know exactly how long a tick was attached. In many cases, the tick is no longer available for identification or testing. People may also be bitten while traveling and never realize where the exposure occurred.
Because of these uncertainties, ILADS believes treatment decisions should not rely solely on estimates of attachment time or geographic location.
Based on its review of the available evidence, ILADS recommends against the IDSA's use of one pill of doxycycline following a known blacklegged tick bite. Instead, ILADS recommends discussing treatment with the patient and, when appropriate, prescribing a 20-day course of doxycycline.4
ILADS believes early treatment provides the best opportunity to prevent Lyme disease from becoming established.
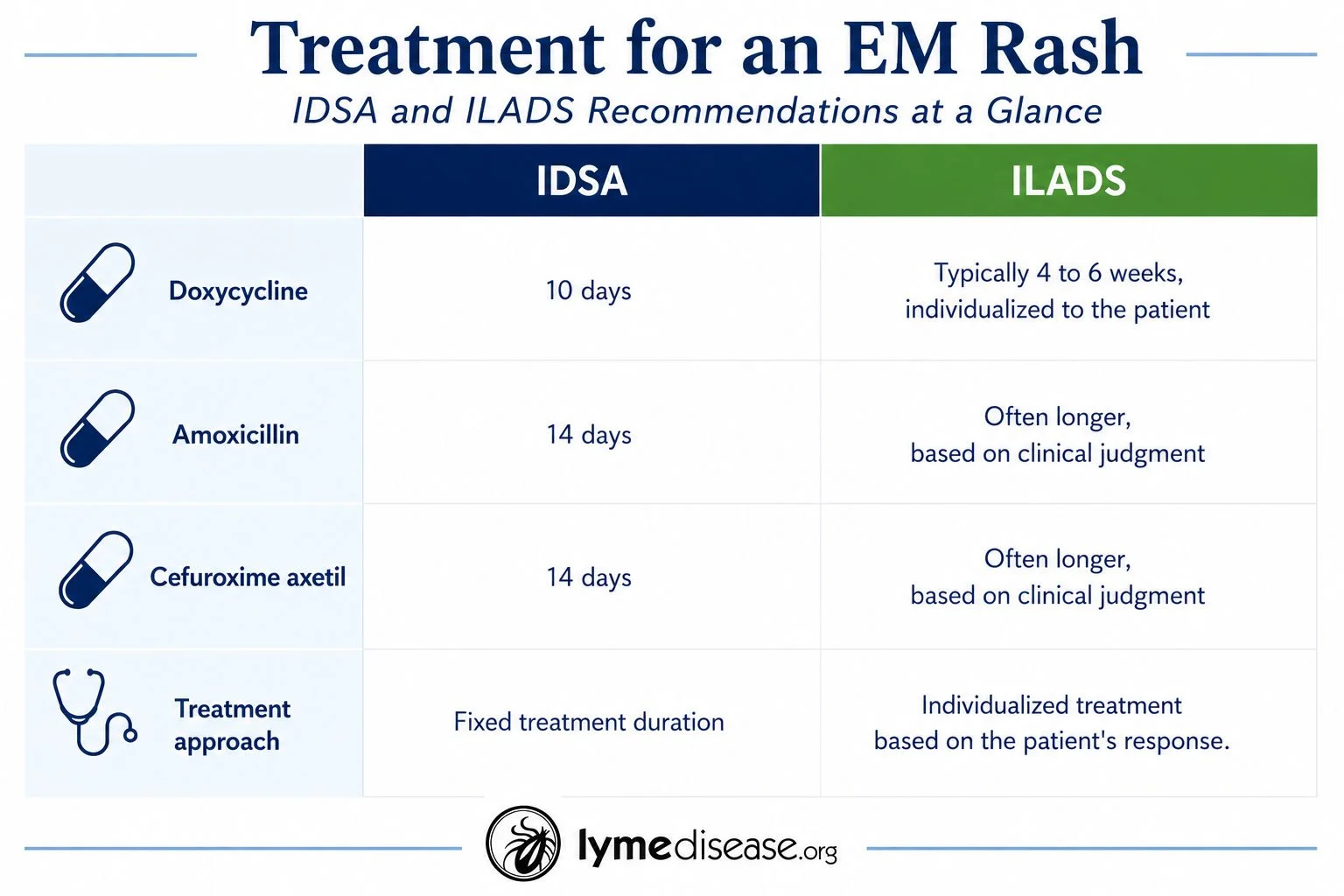
When a rash means Lyme disease
Once an erythema migrans (EM) rash develops, prevention is no longer the goal.
An EM rash is diagnostic of Lyme disease.1 Treatment should begin immediately without waiting for laboratory testing because blood tests are often negative during the earliest stages of infection.1,5
Both the IDSA and ILADS agree on this point. They differ, however, in how long they recommend treating early Lyme disease.1,4
Recognizing an EM Rash
Many people expect Lyme disease to produce a classic bull's-eye rash.
In reality, that appearance is much less common than many people realize.
An EM rash is often:5
Solid red rather than a bull's-eye
Round or oval
Expands over several days
Larger than two inches across
Only mildly itchy or tender
Mistaken for a spider bite or skin irritation
Just as importantly, many patients never notice a rash at all. According to MyLymeData, the largest patient registry for Lyme disease, 55% of participants did not recall having an erythema migrans (EM) rash.7
If you develop flu-like symptoms, fever, fatigue, muscle aches, headaches, joint pain, or other unexplained symptoms after a tick bite, seek medical evaluation promptly, even if you never noticed a rash.
Recognizing what an EM rash can look like, and understanding that many patients never develop one, is an important part of early diagnosis.
A personal perspective
My family's experience is one reason I believe patients should understand both treatment approaches.
In 2015, my son developed heart pain and what looked like a scratch mark rash after a tick bite. We immediately went to our local emergency department, where he received one pill of doxycycline, the treatment commonly recommended under the IDSA guidelines.
The rash stopped expanding, and we hoped the infection had been prevented. Instead, over the following weeks he became increasingly ill and developed a long list of symptoms.
About eight weeks later, he was diagnosed by an ILADS doctor with Lyme disease, Bartonella, and other tick-borne infections. By then, the infections had spread throughout his body.
Every patient's experience is different, and no one can say with certainty what would have happened had another treatment approach been used. What I do know is that our family's experience taught me the importance of understanding that more than one set of medical guidelines exists after a tick bite.
My hope is that every patient understands their options, recognizes the importance of early diagnosis and treatment, and has the information needed to make informed decisions with their healthcare provider.
If you would like to learn more about the ILADS approach to treating Lyme disease after a tick bite, or discuss these recommendations with your healthcare provider, you can review the complete ILADS Treatment Guidelines here:
ILADS Treatment Guidelines
https://www.ilads.org/patient-care/ilads-treatment-guidelines/
Terri McCormick is a writer and advocate with LymeDisease.org. She is the author of Being Misdiagnosed: Stories That Reveal the Hidden Epidemic of Lyme Disease. The book is available on Amazon and at TerriMcCormick.com.
Additional Resources
1. Find an ILADS-trained clinician
https://www.ilads.org/patient-care/provider-search/
2. Learn more about erythema migrans (EM) rashes
https://www.hopkinslyme.org/lyme-disease/lyme-disease-signs-symptoms/
3. Download the LymeDisease.org Lyme disease facts brochure
Endnotes
Infectious Diseases Society of America, American Academy of Neurology, and American College of Rheumatology, 2020 Guidelines for the Prevention, Diagnosis and Treatment of Lyme Disease, Clinical Infectious Diseases 72, no. 1 (2021): e1-e48. https://doi.org/10.1093/cid/ciaa1215.
Centers for Disease Control and Prevention, "Lyme Disease Prophylaxis After Tick Bite," last reviewed December 19, 2024. https://www.cdc.gov/lyme/resources/pdfs/lyme-pep-low-ink-p.pdf.
Centers for Disease Control and Prevention, "Lyme Disease Surveillance and Available Data." https://www.cdc.gov/lyme/data-research/facts-stats/index.html.
International Lyme and Associated Diseases Society, Evidence Assessments and Guideline Recommendations in Lyme Disease: The Clinical Management of Known Tick Bites, Erythema Migrans Rashes and Persistent Disease, Expert Review of Anti-infective Therapy 12, no. 9 (2014): 1103-1135.
Johns Hopkins Lyme Disease Research Center, "Lyme Disease Signs and Symptoms." https://www.hopkinslyme.org/lyme-disease/lyme-disease-signs-symptoms/.
Infectious Diseases Society of America, The Clinical Assessment, Treatment, and Prevention of Lyme Disease, Human Granulocytic Anaplasmosis, and Babesiosis: Clinical Practice Guidelines by the Infectious Diseases Society of America, Clinical Infectious Diseases 43, no. 9 (2006): 1089-1134. https://doi.org/10.1086/508667.
Johnson L, Shapiro M, Needell D, Stricker RB. "Optimizing Exclusion Criteria for Clinical Trials of Persistent Lyme Disease Using Real-World Data." Healthcare 13, no. 1 (2025): 20. https://doi.org/10.3390/healthcare13010020.